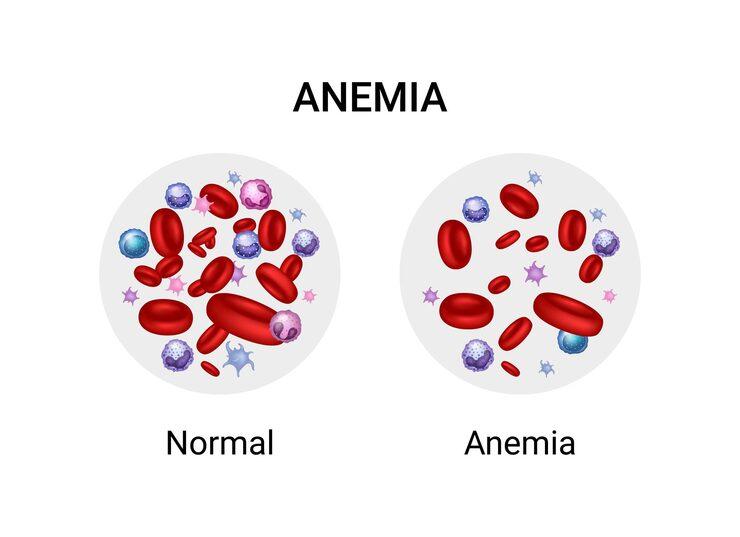
an illustration portraying the difference between anemia and normal blood
It is called a "silent epidemic" for a reason. Unlike thalassemia, which is spread across many Indian communities, sickle cell anemia in India has historically been concentrated in tribal and disadvantaged populations — communities that are geographically remote, politically underrepresented, and medically underserved. For decades, this concentration meant that the disease was largely invisible in mainstream public health discourse.
That invisibility has cost lives. And it continues to cost them.
India is home to one of the world's largest populations of people living with sickle cell disease (SCD). The government's National Sickle Cell Anaemia Elimination Mission, launched in 2023, has acknowledged this reality with a target to eliminate the disease by 2047. But elimination is a long-term goal. In the meantime, hundreds of thousands of patients need regular blood transfusions to survive — and that blood has to come from somewhere.
Sickle cell anemia is an inherited blood disorder. It is caused by a mutation in the gene that codes for haemoglobin — the protein in red blood cells that carries oxygen.
In a person with sickle cell anemia (the homozygous HbSS form), the haemoglobin produced is structurally abnormal. Under low-oxygen conditions — during physical stress, illness, dehydration, or cold exposure — this abnormal haemoglobin causes red blood cells to change shape. Instead of the smooth, disc-like shape that allows red blood cells to flow freely through blood vessels, they become rigid and crescent-shaped — like a sickle.
These sickled cells:
Sickle cell disease in India is primarily — though not exclusively — a disease of tribal and indigenous communities.
The states with the highest burden are:
A 2024 study published in the International Journal of Community Medicine and Public Health noted that between 10% and 30% of tribal groups in Madhya Pradesh and Chhattisgarh carry the sickle cell trait — making these the most affected populations in the country.
The sickle cell trait (HbAS) — being a carrier of one copy of the gene — is far more prevalent than the disease itself. Carriers typically have no significant health problems but can pass the gene to their children. When two carriers have a child, there is a 25% probability with each pregnancy that the child will have sickle cell disease.
Not all sickle cell patients require regular blood transfusions. The severity of SCD varies significantly, partly because many Indian tribal patients also carry alpha-thalassemia or have elevated foetal haemoglobin levels, which can moderate the course of the disease.
Emergency transfusions during acute crises:
Chronic transfusion programmes:
For high-risk patients — particularly children who have had strokes or show abnormal transcranial Doppler velocity — regular monthly transfusions reduce the risk of recurrence. These programmes require the same sustained, long-term blood supply as thalassemia management.
Pre-operative transfusions:
Before major surgical procedures, many SCD patients receive transfusions to reduce the proportion of sickle haemoglobin in their blood, reducing perioperative risk.
Geographic remoteness: The communities most affected by SCD in India — tribal populations in Chhattisgarh, MP, Odisha, and Gujarat — often live far from blood banking infrastructure. A BMJ Global Health study found that in eight EAG states (which include Chhattisgarh, Odisha, and MP), only 26% of residents live within 30 minutes of a blood bank. For rural tribal populations, the distance is even greater.
Replacement donation pressure: Without a strong voluntary donor base in these communities, families of SCD patients must scramble for replacement donors each time a transfusion is needed. This is emotionally exhausting, logistically difficult, and clinically inferior to planned, voluntary donation.
Alloimmunisation risk: As with thalassemia, SCD patients who receive many transfusions over time can develop antibodies against minor blood group antigens in donated blood. Once alloimmunised, compatible blood becomes significantly harder to find. This reinforces the need for extended blood typing and antigen-matched transfusions — a standard that most blood banks in India, particularly in smaller towns, cannot yet meet.
Infection risk: Patients who receive blood from replacement donors — often donating under pressure, potentially concealing health risks — face higher exposure to transfusion-transmitted infections than those receiving blood from screened voluntary donors.
In June 2023, Prime Minister Narendra Modi launched the National Sickle Cell Anaemia Elimination Mission in Shahdol, Madhya Pradesh — a tribal district with high SCD prevalence. The mission aims to:
This is a significant policy commitment. But the mission's success depends partly on something it cannot mandate: a reliable, voluntary blood supply for the patients already living with the disease today.
Every voluntary blood donor who gives blood every 90 days (men) or 120 days (women) contributes to the pool from which SCD patients draw their transfusions. The more robust and geographically distributed this pool, the more reliably SCD patients across India — including in smaller towns closer to tribal populations — can access blood.
Blood donation camps in tier-2 and tier-3 cities closest to SCD-endemic regions are particularly impactful. If you live in Raipur, Jagdalpur, Berhampur, Nagpur, Surat, or similar cities near high-prevalence tribal areas, your donation is disproportionately valuable.
Sickle cell disease is under-discussed in mainstream Indian health conversations. Sharing accurate information — particularly about the need for voluntary blood and the risks of leaving SCD untreated — helps build the social awareness that supports both donations and disease screening.
TheBloodApp enables urgent blood requests from SCD patients and their families — including in smaller cities and towns where hospital blood banks may be stretched thin. A registered voluntary donor in Raipur or Bhubaneswar responding to an urgent SCD transfusion alert through the app is closing a gap that institutional systems cannot close on their own.
Register on TheBloodApp. Donate regularly. If you live near a tribal or rural community with high SCD prevalence, your blood has a direct path to someone who needs it month after month. To find donation camps near you or to submit an urgent blood request, call the number listed in the app.
Sources: PMC — Sickle Cell Disease in Tribal Populations in India | PMC — Sickle Cell Anemia Chhattisgarh Screening | International Journal of Community Medicine and Public Health — SCD Burden in India 2024 | Nature Scientific Reports — SCD Epidemiology Rajasthan 2025 | WHO India Blood Safety Report 2024 | MoHFW — National Sickle Cell Anaemia Elimination Mission | PLOS ONE — India Blood Demand Study
Stay informed, stay inspired — your go-to source for everything about blood donation and impact.

India has the world's largest vegetarian population — and millions of eligible vegetarian blood donors who worry about low iron. Here's the complete, science-backed guide to staying eligible as a vegetarian donor.

Billoo Ji from Assam has donated blood 114 times. Gujarat has over 225 centurion donors. Meet the remarkable Indians who made blood donation a lifetime habit — and what their stories teach us.

Tripura achieves 95% voluntary donation. Thirteen Indian states are below 50%. Here's the complete state-by-state picture of India's blood donation landscape — and what the gaps cost patients.
Be a part of the change — donate safely, stay connected, and help someone in need. Download the app today.
Available on